NEUROMODULATION THERAPY · IMPLANTABLE · REVERSIBLE · NON-OPIOID
What Is Spinal Cord Stimulation (SCS)?
Spinal cord stimulation is a form of neuromodulation — a rapidly advancing field that uses implantable devices to deliver precisely targeted electrical signals to the nervous system, modifying how the brain perceives pain rather than masking it with medication.
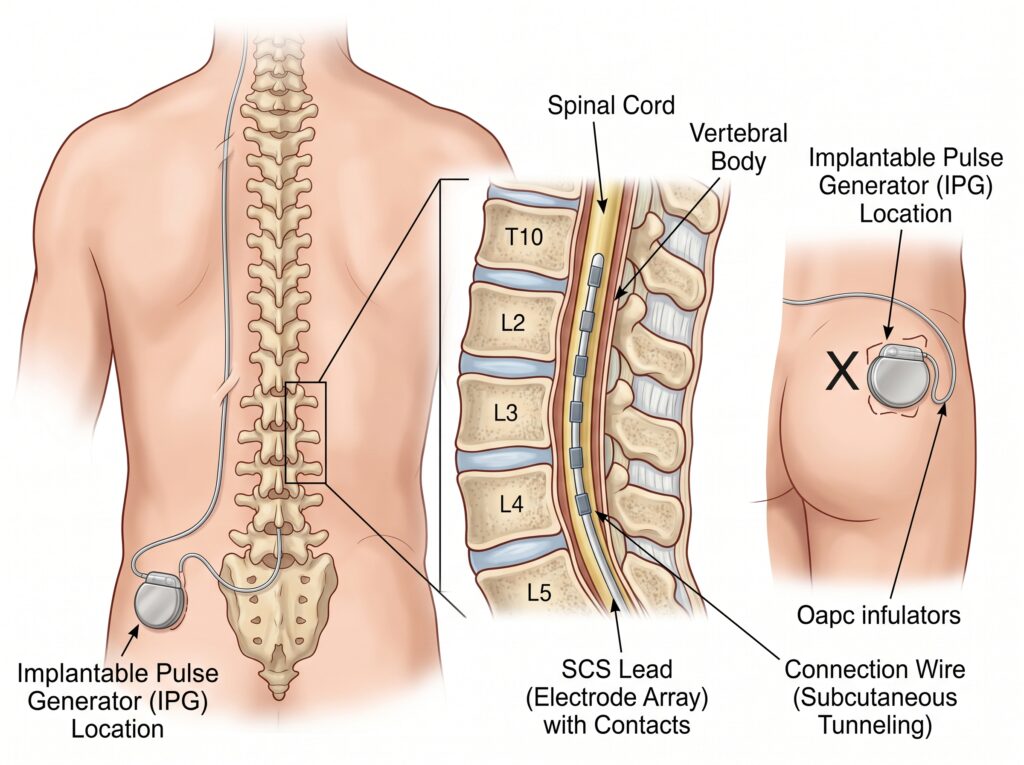
Unlike conventional analgesics, SCS works by delivering low-voltage electrical pulses to neural targets within the dorsal epidural space of the spinal cord. These pulses interrupt and modify pain signals travelling toward the brain, effectively reducing chronic pain intensity for conditions that have failed all other treatments.
A landmark nationwide analysis in the USA found that SCS for refractory chronic pain can significantly reduce opioid use, opioid-related morbidity and mortality, and the enormous economic burden associated with long-term opioid therapy — making it a critical tool in the modern pain specialist’s armamentarium.
Neuromodulation as a field is broadly divided into Intrathecal Drug Delivery Systems and Neurostimulation Therapies, of which SCS is the most widely used and evidence-backed modality for chronic neuropathic pain.
HOW IT WORKS
The Three Components of an SCS System
A complete spinal cord stimulation system consists of three precisely engineered components working in concert to deliver individualised pain relief.
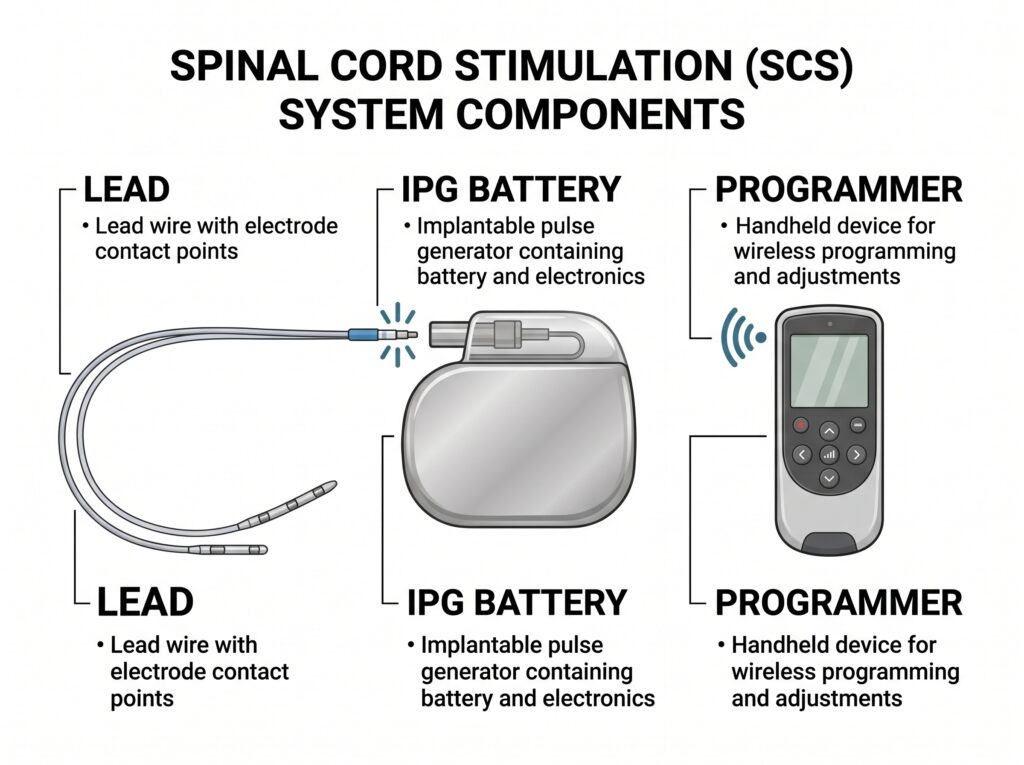
① The Lead
A thin, insulated wire (or flat plate) with 4 to 32 metal contact points — each no larger than a grain of rice. The lead is placed in the dorsal epidural space and delivers targeted electrical pulses directly to spinal cord neural targets. Leads are available in percutaneous (cylindrical) and paddle (flat plate) designs, selected according to the patient’s anatomy and pain distribution.
② The Implantable Pulse Generator (IPG)
The energy source of the system — approximately the size of a stopwatch. Available as:
- Rechargeable: requires an external wireless charger; longer device lifespan
- Non-rechargeable: lithium-based; no charging needed; replaced when battery depletes
The IPG is implanted in a small pocket under the skin, typically in the gluteal region or abdominal wall.
③ The Programmer
A portable device that tailors stimulation parameters — frequency (Hz), pulse-width (μs), and amplitude (mA or V) — to each patient’s individual pain pattern. Separate patient-use and physician-use versions offer flexible, day-to-day control. Modern programmers communicate wirelessly with the IPG.
PATIENT SELECTION
Who Benefits from Spinal Cord Stimulation?
SCS is considered when chronic pain has not responded adequately to conservative treatments. Careful patient selection — ideally through a multidisciplinary team — is the foundation of a successful outcome.
| Primary (Established) Indications | Secondary Indications (Encouraging Evidence) |
| → Failed Back Surgery Syndrome (FBSS) → Complex Regional Pain Syndrome — Type I & II → Peripheral Vascular Disease with ischaemic pain | → Phantom limb pain → Refractory angina (not amenable to revascularisation) → Post-herpetic neuralgia → Severe diabetic peripheral neuropathy |
| Expanding Indications (Active Research) | Pre-Implant Assessment Essentials |
| → Migraine & Occipital Neuralgia → Post-surgical pain syndromes → Visceral pain — Chronic Pancreatitis → Chronic non-surgical abdominal pain | → Multidisciplinary team evaluation → Exclusion of major psychiatric comorbidity → Latest imaging for anatomical detail → Realistic outcome expectations established |
THE PROCEDURE
SCS Implantation: A Two-Stage, Reversible Process
SCS implantation is a non-destructive, fully reversible therapy. It follows a two-stage protocol specifically designed to confirm benefit before committing to permanent implantation — giving both patient and physician the confidence of objective evidence.
| STAGE 1 · 3–7 Days Trial Stimulation Leads with stimulating electrodes are placed in the dorsal epidural space and connected to an external trial stimulator. You keep a detailed pain diary during this period. ✓ Success criterion: ≥50% reduction in pain intensity. Failure? Leads are simply removed — no permanent changes to your body. | STAGE 2 · Permanent IPG Implantation Following a successful trial, the Implantable Pulse Generator (IPG) is placed in a small subcutaneous pocket in the gluteal or abdominal region, then connected to the permanent leads. ✓ Recovery: Most patients resume normal activities within a few weeks. Programming is personalised in follow-up sessions. |

Important: The rate of SCS success is inversely proportional to the time elapsed between chronic pain onset and implantation. Early referral to a high-volume specialist centre significantly improves long-term outcomes.
CLINICAL PROFILE
Advantages & Limitations of SCS Therapy
| Key Advantages | Considerations & Limitations |
| → Non-pharmacological: critical alternative amid the opioid crisis → Fully reversible — no anatomical alteration to the nervous system → Provides long-term effective pain relief → Programmable for truly individualised treatment → Cost-effective over 3–4 years vs. ongoing analgesics → Reduces dependence on multiple medications | → Higher upfront device cost (long-term cost-effectiveness established) → Outcome quality is closely tied to centre expertise and programming skill → Hardware-related issues (lead migration) occur in a minority of cases → Stimulation tolerance can develop; newer waveforms are addressing this → Requires ongoing follow-up and programming adjustments |
Evidence Base & Clinical Outcomes
The evidence for SCS continues to grow. For Failed Back Surgery Syndrome (FBSS) — the most studied indication — the evidence meets best-practice synthesis criteria for Level I to II efficacy, based on multiple high-quality randomised controlled trials.
| Level I–II Evidence level for SCS in lumbar FBSS (three high-quality RCTs) | Level II–III Evidence for high-frequency stimulation (one high-quality RCT) | Cost-Effective Systematic review confirms cost-effectiveness vs. conventional care long-term |
A comprehensive systematic review consistently showed SCS to be cost-effective over long-term horizons, particularly for FBSS and Complex Regional Pain Syndrome. Further cost-effectiveness data is accumulating for ischaemic pain and diabetic peripheral neuropathy.
Adaptive stimulation and burst stimulation modalities currently have more limited evidence, and future research should focus on identifying patient phenotypes most likely to benefit from specific waveform technologies.
Newer Advances in Spinal Cord Stimulation
The SCS landscape is evolving rapidly. Research into novel waveforms, targets, device technologies and programming techniques is expanding the therapy’s reach and improving long-term outcomes.
| ⚡ Novel Waveforms & Frequencies High-frequency and burst waveforms stimulate below perception threshold and are addressing tolerance, with promising results in prospective trials. Sub-perception stimulation eliminates uncomfortable paraesthesiae in many patients. | 🎯 New Anatomical Targets Dorsal Root Ganglion (DRG) stimulation and stimulation of the medial branch of the dorsal ramus offer more selective pain modulation, particularly for focal pain syndromes. |
| 🔋 Power & Device Technology Novel implantable power technologies — including skin-based power sources — are extending device longevity. Improved MRI compatibility is enabling full-body MRI access for patients with implanted SCS systems. | 🧠 Closed-Loop & Adaptive Systems Next-generation devices incorporate sensors that respond in real time to patient movement and posture, delivering consistently optimised stimulation throughout daily activities. |
Our Approach: What Sets Our Results Apart
Successful SCS outcomes are inseparable from the expertise of the implanting centre. Our programme incorporates every recognised factor associated with superior, durable pain relief.
| Patient Selection Rigorous multidisciplinary assessment to identify ideal candidates | Patient Education Thorough pre-procedure counselling for patients and families | Psychiatric Screening Rule-out of major psychiatric comorbidity before proceeding |
| Advanced Imaging Latest imaging for precise anatomical planning and lead placement | Timely Referral Early SCS application — earlier implantation yields better long-term success | Meticulous Technique Precision implantation with optimal lead selection and positioning |
| Programming Mastery Individualised, expert post-implant programming optimisation | Holistic Rehabilitation ngoing physical and psychological support alongside SCS therapy | Long-term Follow-up Structured follow-up programme to ensure sustained benefit |
FREQUENTLY ASKED QUESTIONS
| Q: Is spinal cord stimulation painful? The implantation procedure is performed under sedation or local anaesthesia and is generally well tolerated. Post-operative discomfort is typically mild and managed with standard analgesics. Once active, patients typically feel a gentle tingling or nothing at all, depending on the waveform used. |
| Q: Can I have an MRI after SCS implantation? MRI compatibility varies by device manufacturer and model. Many modern SCS systems are now conditionally MRI-compatible under specific conditions. Your physician will advise on the specific restrictions relevant to your implant. |
| Q: What if the SCS trial does not work? If the trial stimulation fails to achieve the required 50% reduction in pain intensity, the leads are simply removed in a minor procedure, leaving no permanent changes. There are no residual or after-effects, and alternative treatment strategies can then be explored. |
| Q: How long does an SCS system last? Non-rechargeable IPG batteries typically last 3–5 years depending on usage; rechargeable systems can last 8–10 years or more. The leads themselves are designed for long-term use. Battery replacement is a minor day-procedure. |
| Q: Does SCS replace all other pain medications? SCS significantly reduces — and in many patients eliminates the need for — opioid medications. Many patients are able to substantially taper their analgesic use, reducing drug-related side effects and improving overall quality of life. Your pain management plan is tailored individually. |
| Q: Who is a good candidate for SCS? Ideal candidates have chronic neuropathic pain (particularly FBSS or CRPS), have failed conservative treatments, have no major untreated psychiatric comorbidity, and have realistic expectations. A multidisciplinary team assessment at our centre will determine suitability. |
Ready to Explore SCS for Your Chronic Pain?
Our specialist pain team has two decades of SCS experience. Book a consultation to find out if you are a candidate for this life-changing therapy.
Request a consultation call now on 91 22 66573076 [9am-5pm]